

Jaw Growth, Facial Development, and Sleep in Children
What Can We Do — and When?

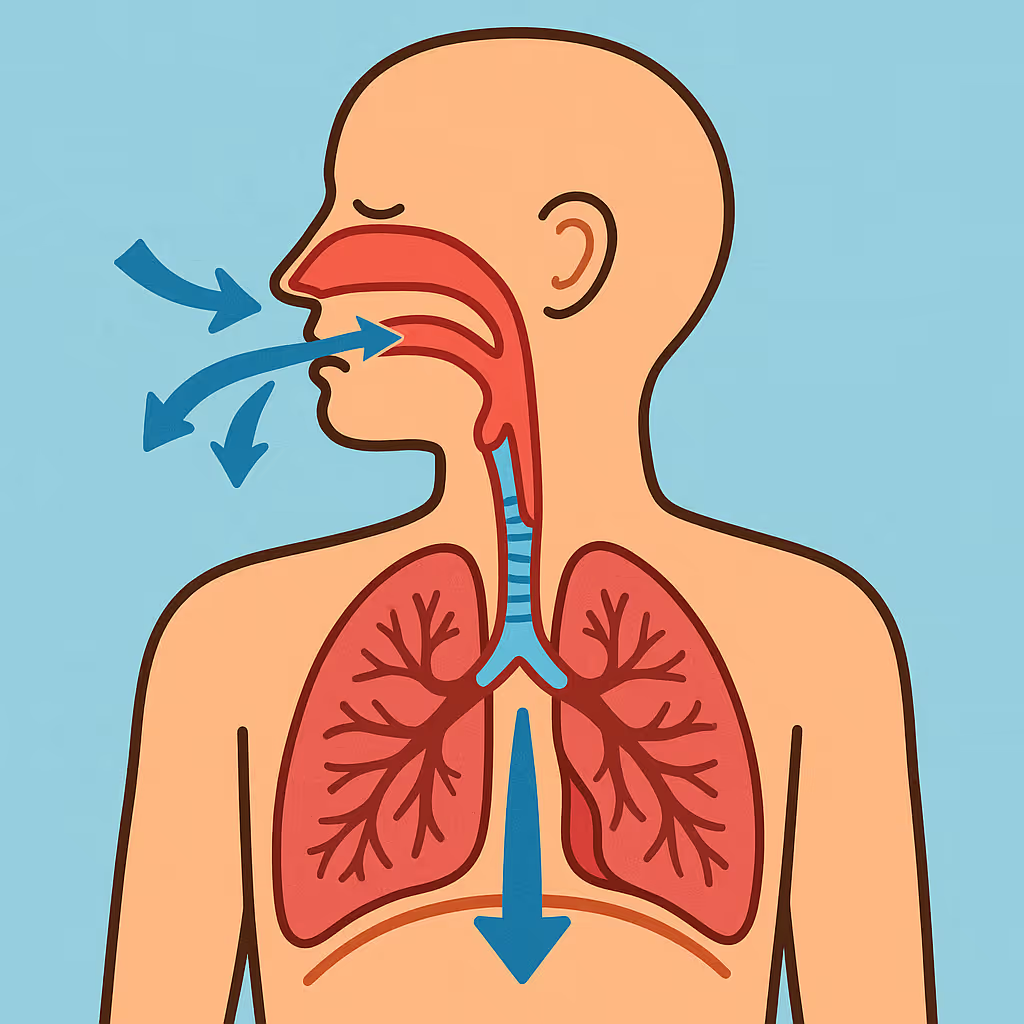
Understanding Sleep-Disordered Breathing in Children
Sleep-disordered breathing (SDB) exists on a spectrum. It can range from:
• simple snoring
• increased breathing effort during sleep
• to obstructive sleep apnea (OSA)
When untreated, SDB can affect a child’s:
• sleep quality
• daytime behavior and attention
• learning and academic performance
• growth hormone release
• cardiovascular and metabolic health
Unlike adult sleep apnea, pediatric SDB is often developmental in nature — meaning it evolves as the child’s face, jaws, and airway grow.

The Role of Craniofacial Growth
The reviewed literature emphasizes that craniofacial structure and growth patterns strongly influence airway size and stability.
Certain facial and jaw patterns increase the likelihood that the airway will narrow or collapse during sleep, especially when muscle tone decreases at night.
These craniofacial phenotypes include:
• Narrow maxilla (upper jaw constriction)
• Retrognathic mandible (small or retruded lower jaw)
• Vertical maxillary excess
• Midface hypoplasia
• Other skeletal variations affecting airway dimensions
These structural patterns do not simply affect facial aesthetics — they directly influence airflow, tongue posture, and airway patency.
More Than Anatomy Alone
Importantly, the article highlights that airway collapse is rarely caused by anatomy alone.
Both anatomic and non-anatomic factors contribute, including:
• enlarged tonsils and adenoids
• chronic inflammation
• nasal obstruction
• reduced neuromuscular control during sleep
When these factors coexist with an unfavorable jaw structure, the risk of sleep-disordered breathing increases significantly.


Identifying Risk Through Craniofacial Phenotyping
A major focus of the review is the concept of craniofacial phenotyping — identifying specific structural patterns of the face and jaws that predispose children to airway compromise.
By recognizing these phenotypes early, clinicians can:
• identify children at higher risk for SDB
• understand where airway collapse is most likely occurring
• choose the most appropriate timing and type of intervention
This approach moves away from a “one-size-fits-all” model and toward individualized, growth-guided care.
Timing Matters: Why Early Intervention Is Critical
Facial growth does not occur evenly throughout childhood. There are critical windows of opportunity during which orthopedic and orthodontic interventions can guide skeletal development more effectively.
The article outlines how treatment strategies should be selected based on:
• which skeletal structure is deficient
• the direction of growth needed (transverse, anteroposterior, or vertical)
• the child’s stage of dental and skeletal maturity
When intervention is timed correctly, orthodontic treatment can do more than align teeth — it can support healthier airway development.


A Shift in How We View Early Orthodontics
This research reinforces a powerful message:
Early orthodontics is not just about moving teeth.
Teeth are often the most visible sign of an underlying problem, but the deeper issue frequently lies in:
• jaw growth
• facial balance
• airway function
Sleep-disordered breathing in children is dynamic — it changes as the face grows. Our responsibility as clinicians is not to treat every child the same way, but to recognize the growth pattern in front of us and understand how it may influence breathing, sleep, and long-term health.
The Importance of a Multidisciplinary Approach
Optimal care for children with sleep-related breathing concerns requires collaboration.
The article emphasizes a multidisciplinary model, involving:
• pediatric dentists
• orthodontists
• ENT specialists
• sleep medicine professionals
By working together, teams can optimize both timing and choice of intervention, ensuring that treatment supports not only dental alignment, but also airway health and physiological development.


Final Thoughts
Children do not outgrow airway problems — they grow into them.
By identifying craniofacial patterns early and understanding their relationship to sleep and breathing, clinicians have the opportunity to intervene at the right time, with the right strategy, for the right child.
Early orthodontic care, when guided by growth and function, becomes a powerful tool — not only for smiles, but for sleep, health, and lifelong well-being.
Orthodontic Techniques That Support Airway and Jaw Development
When applied at the appropriate stage of growth, orthodontic treatment can play a meaningful role in supporting both jaw development and airway function.
The reviewed literature highlights that different orthodontic modalities influence craniofacial structures in different ways. Therefore, treatment selection must be individualized and guided by the child’s growth pattern rather than chronological age alone.
Techniques commonly used in growth-guided and airway-focused orthodontics include:
Functional Appliances
Functional appliances are designed to guide mandibular growth and improve jaw relationships during active growth phases. By encouraging forward positioning of the lower jaw, these appliances may help increase the space available for the upper airway in selected patients.
They are most effective when used during periods of active skeletal development, particularly in children with mandibular retrusion associated with sleep-disordered breathing.
Maxillary Expansion Devices
Transverse maxillary constriction is one of the most frequently observed craniofacial phenotypes associated with pediatric sleep-disordered breathing.
Expansion devices — including slow expansion and rapid palatal expansion — aim to widen the upper jaw, which can:
• increase nasal cavity volume
• reduce airway resistance
• improve tongue posture
• support nasal breathing
When used during growth, expansion addresses not only dental crowding but also the skeletal foundation of the midface.
Aligner-Based and Adjunct Orthodontic Modalities
Clear aligners and other orthodontic systems may be used as part of a comprehensive treatment plan to support dental alignment while maintaining or enhancing functional goals.
When combined with appropriate orthopedic strategies, these modalities can contribute to overall treatment stability and functional balance.

The Importance of Timing
A critical message emphasized in the article is that the effectiveness of these techniques is closely tied to timing.
Applied too early or too late, the same appliance may produce very different outcomes. When used during optimal growth windows, however, orthodontic interventions can support:
• favorable jaw development
• improved airway dimensions
• long-term functional stability
This reinforces the importance of early assessment and continuous monitoring of craniofacial growth rather than delaying evaluation until permanent teeth are fully erupted.
The skilled hands that care for your smile









She has practiced in both private clinics and hospital-based settings in North America, the Middle East, and GCC countries. Her practice blends modern pediatric dentistry, with her own expansion protocols in interceptive orthodontics, and myofunctional therapy to address the root causes of dental and airway issues in growing children, and revolves around a multi-disciplinary team of ENT doctors, speech and feeding therapists, sleep surgeons and physiotherapists. She is also highly skilled in treating and managing special needs children and has played a significant role in raising oral health awareness in the Middle East and GCC region through various media channels, conferences and
She is also the author of the children’s book “Danny and Sarah Go to Dr. Smile,” which helps children overcome dental anxiety through an engaging and reassuring story — reflecting her commitment to making dental care a positive, empowering experience.
A proud mum of three, Dr. Tayara combines her professional expertise with a deeply personal understanding of what families need — creating an environment where every child feels safe, understood, and cared for. Her mission is simple yet powerful: to help children breathe, grow, and smile better for life.
You can find her on:
Instagram @doctortayara.
LinkedIn @doctortayara.
Linktr @doctortayara.
Website @doctortayara.

Dr. Micheline brings warmth, expertise, and a deep passion for children’s oral health. As a mom of two herself, she understands how to make every child feel safe, heard, and comfortable at the dentist.
She specializes in a full range of pediatric dental treatments including crowns, fillings, pulp therapy, laughing gaz, and general anesthesia (GA) for more complex cases. She is also a certified Invisalign First provider, offering early orthodontic solutions for growing smiles.

Frequently asked questions












